
Mesh Complications Patient Story 25
Severe Vaginal Pain following TOT Sling and Posterior Vaginal Mesh Procedure
Mesh Complications: Severe vaginal and buttock pain, severe pain with intercourse, vaginal bleeding, and mesh extrusion
Treatment: Posterior vaginal mesh removal, TOT sling removal
The patient is a 56 -year- old woman who had surgery by her gynecologist for a cystocele and rectocele three years ago. She had an Avaulta (C. R. Bard) mesh repair for her rectocele and a TOT sling for incontinence.
After surgery, the patient reported a great deal of vaginal and pelvic pain. She began having vaginal bleeding and upon follow up was found to have mesh extrusion through the posterior vaginal wall. She was told by her physician, “These things just take time to heal.” The patient reported feelings of frustration at the lack of support from her healthcare provider.
Her pain persisted and over time moved to her lower back and buttocks with reports of intense vaginal pressure. The patient reported difficultly driving or sitting for long periods of time. She could not walk or exercise, and the pain was waking her up at night She attempted intercourse three times, however, could not tolerate it secondary to extreme pain.
Bard Avaulta Mesh
The patient is a 56 -year- old woman who had surgery by her gynecologist for a cystocele and rectocele three years ago. She had an Avaulta (C. R. Bard) mesh repair for her rectocele and a TOT sling for incontinence.
The patient consulted Drs. Moore and Miklos. Examination of the patient revealed the sling and the lateral arms of the posterior Avaulta mesh were under tension and pulling on the vaginal sidewall muscles. Palpation of these arms caused severe pain to the patient.
Drs. Moore and Miklos surgically removed the vaginal portion of the TOT sling and then removed the bulk of the posterior vaginal wall mesh by cutting the largest portion of the mesh away from its anchoring arms, which remained in the patient’s body. The patient’s pain most likely was generated from the tension on the muscles the sling and the arms of the mesh were causing. Usually removing the tension helps to relieve the majority of the pain.
Comment by Dr. Moore: The mesh arms of any posterior system of the first generation mesh kits utilizing trocars or needles to place them through the groin or buttock cheeks typically do not need to be removed unless they are infected. The pain is typically secondary from the arms pulling on the muscles from the vaginal side, and it usually is only necessary to remove the arms up to the point they attach to the muscle. This releases the tension and often the pain improves. The newer generation mesh procedures such as Elevate and Pinnacle do not use this type approach and seem to have fewer issues with pain. The mesh itself is not causing the problem or pain; it is how it is placed, how it heals, or how the arms are pulling on the muscles that may be causing the pain. Vaginal mesh used for prolapse that is placed correctly in the right patient by an advanced pelvic surgeon will have very low rates of complications and the advantages of high cure rates.
The patient has recovered well, and though she still has some pain, the pain down the back of her leg and in her buttock cheek has completely dissipated. The pulling pain in her vagina has resolved. She is undergoing pelvic floor physical therapy and has a positive outlook for pain free intercourse in the future.
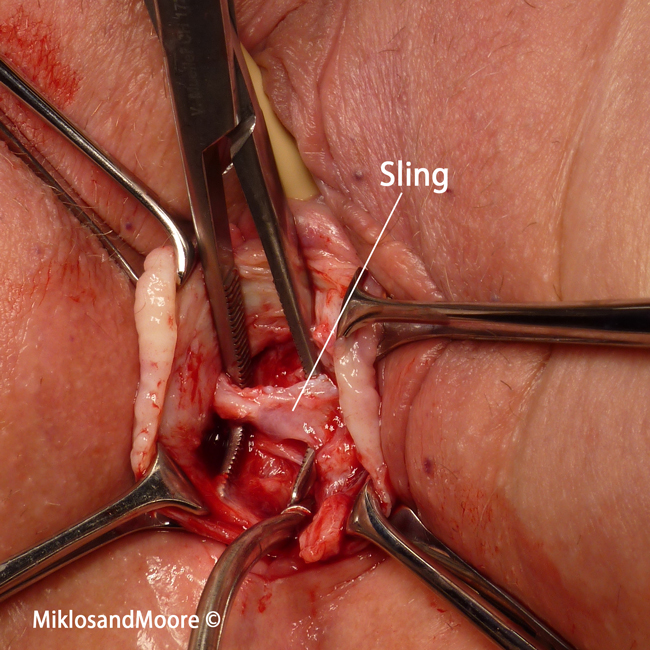
Picture 1 - Mesh tape from sling isolated prior to removal
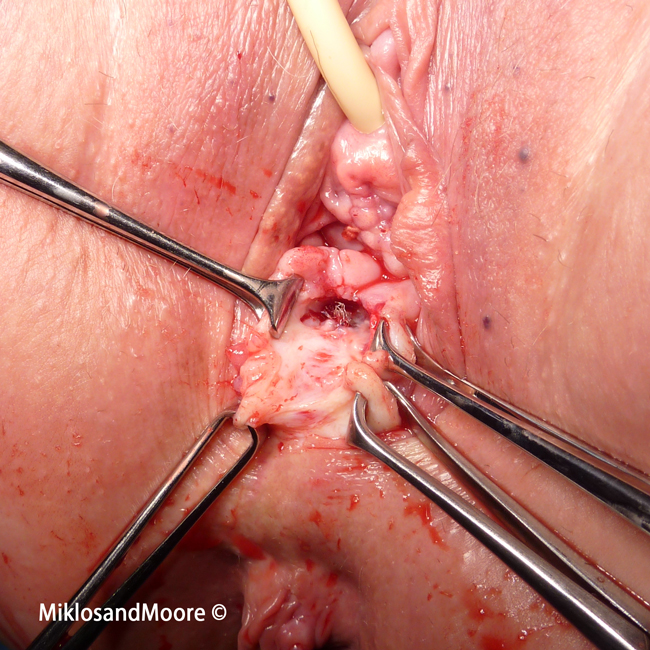
Picture 2 - Mesh frayed where it had extruded through vagina
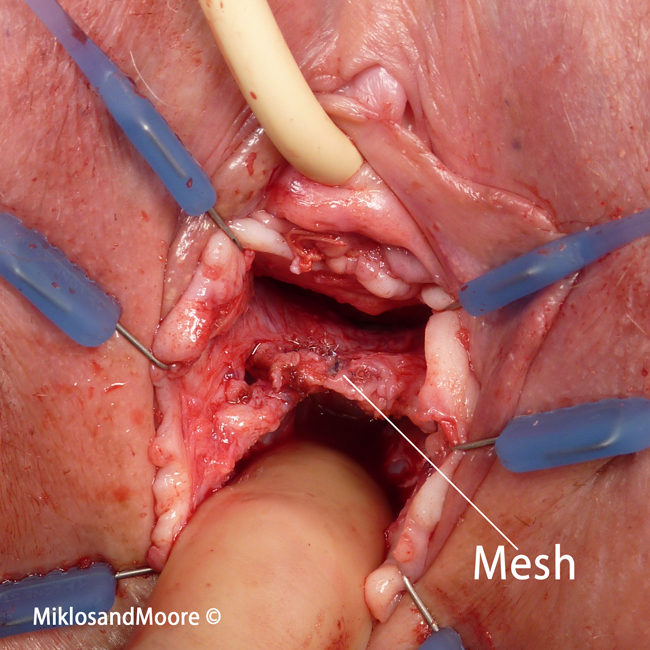
Picture 3 - Post wall mesh isolated at beginning of dissection
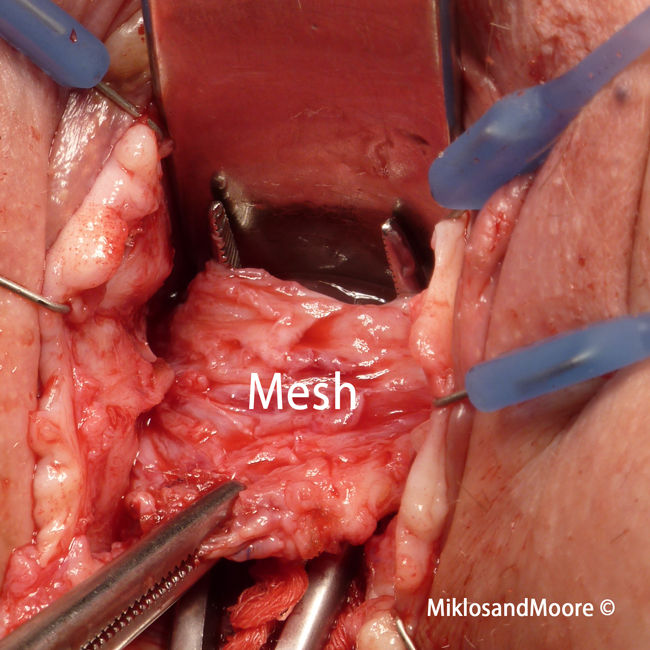
Picture 4 - Post mesh freed up and isolated
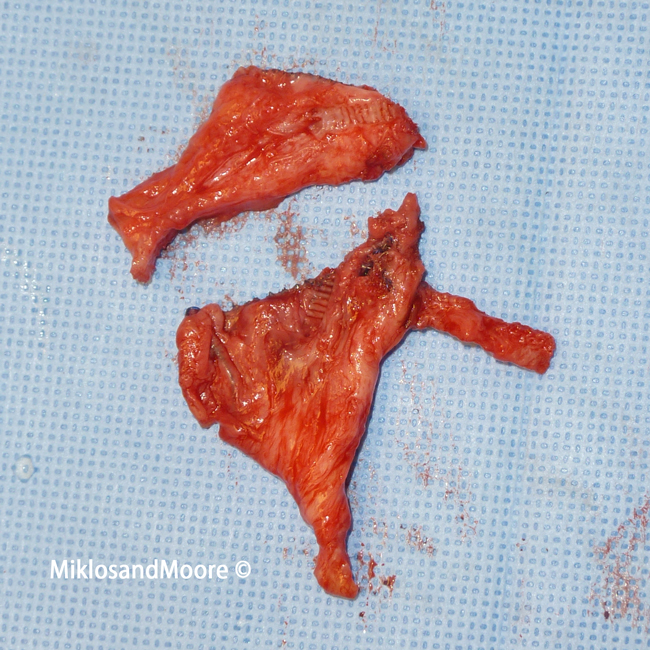
Picture 5 - Post wall mesh removed
Click here to find out more about TOT Sling complications.
Click here to find out more about Avaulta complications.
Click here for related patient stories