
Mesh Complications Patient Story 26
Mesh Extrusion from Posterior Vaginal Wall Mesh
& Lower Abdominal Pain following a TVT Sling
Mesh Complications: Sigmoid colon perforation with TVT sling, vaginal mesh extrusion from posterior vaginal mesh, persistent rectocele and vaginal vault prolapse
Treatment: Laparoscopic and vaginal removal of TVT sling mesh. Removal of previous TVT sling with Bowel Resection. Placement of new TVT sling and Laparoscopic Sacral Colpopexy
The patient is a 62- year- old woman who had surgery five years ago that included a TVT sling for stress urinary leakage (SUI) and a posterior repair with mesh graft (no kit) for a rectocele.
The patient presented with symptoms of persistent urinary leakage with laughing, coughing, or sneezing and a large bulge vaginally causing pressure and discomfort. She stated that the surgery worked for a period of time for the prolapse, but never really helped her SUI. Examination revealed a large rectocele and the posterior wall mesh was gathered (providing no support) into a ball on one side of her vagina. It had also extruded out of the vaginal skin. She also had a vaginal vault prolapse.
Drs. Moore and Miklos took the patient to surgery to remove the previous mesh and repair the prolapse and incontinence. The posterior vaginal mesh was no longer helping her rectocele and was extruding out of the vagina skin. The mesh needed to be removed. Additionally, the TVT sling was not working well for her urine leakage and needed replacement.
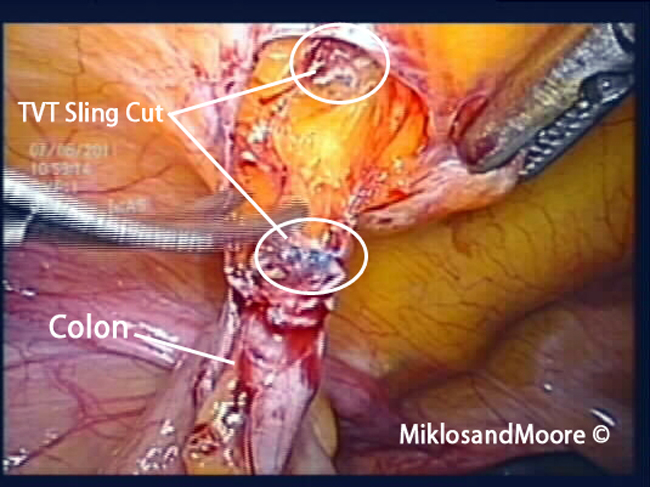
The new TVT was completed at the beginning of the case, and the patient was put to sleep after adjustment. A laparoscopic approach was taken to repair the vaginal vault prolapse by doing a sacral colpopexy. Upon entry into the abdomen, the surgeons found that the patient’s OLD TVT sling was going THROUGH her large intestine (see pictures below). The sling was immediately removed, and the bowel was resected (Sigmoid Colon Resection).
Secondary to the clean nature of the case, the sacral colpopexy was able to be completed, and the patient did very well post-operatively with no infection, no urinary leakage, normal return of bowel function and excellent vaginal support!
***This was a VERY complex case and one that only advanced laparoscopic/pelvic surgeons should consider.
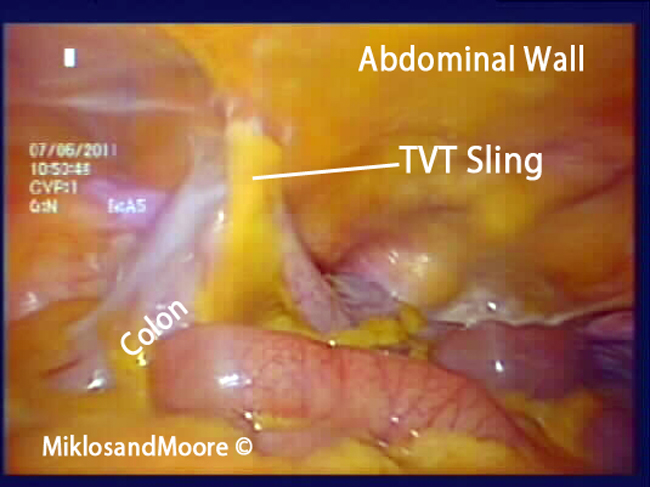
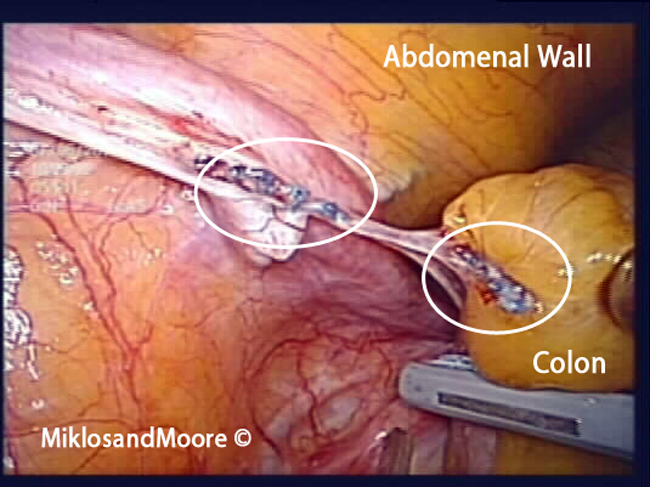
Picture 1: Sigmoid Colon pulled up to the Abdominal Wall
Picture 2: Cutting the mesh away from the Abdominal Wall

Picture 3: Cutting the other side of the bowel and mesh away from the pelvic sidewall
Picture 4: Picture of the released bowel with the old TVT sling going through and through the bowel. This area of bowel had to be removed and resected.

Picture 5 & 6: Pictures of the removed piece of bowel with the TVT mesh penetration.

Picture 6
Click here to find out more about TVT Mesh complications.
Click here for related patient stories