




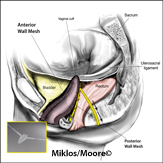
Vaginal Mesh Kits Complications
Mesh has been used for prolapse repair (i.e. vaginal vault prolapse, cystocele and rectocele) for many years. It has been proven to be the most successful repair for vaginal vault prolapse in the literature and is considered standard of care (abdominal mesh sacralcolpopexy). Although considered the standard of care with this procedure, complications can still occur including infection, pain, mesh extrusion through the vagina or erosion into viscera such as the bladder or bowel. More recently it has become more popular to place the mesh vaginally with kits to treat prolapse. As with any new technology there is learning curves both surgically and with technology and this can lead to complications when newer procedures are developed. Additionally, these kits were developed by industry who then trained many surgeons to do the procedures which resulted in many inexperienced surgeons doing them and complications ensued. This led to an FDA notification in the fall of 2008 that notified patients to be aware of the complications that do potentially exist and to ensure your surgeon has the proper training and experience to do the procedures. It has also led to improvement in surgical technique and mesh technology which have both decreased complications as well. There are also many studies supporting the use of mesh placed both abdominally and or vaginally, however again it is very important that it be used in the PROPER patient selection and by surgeons with PROPER training and experience.
Mesh has been proven and shown to have higher cure rates than using the patients own tissue that has already failed, however again it takes a specialist with extra years of training and an expertise in vaginal reconstruction to decide on its appropriate use. The mesh itself DOES NOT cause the complication, how the body reacts to it and how it is placed are the primary causes of complications. It also is important to note that NO surgery is free of risk of complications whether mesh is used or not. For more information about mesh kits please see Drs. Moore and Miklos’s recent published article (Vaginal Mesh Kits: Friend or Foe) and their urogynecological website.
Types of Complications
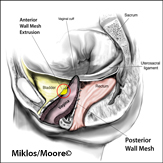
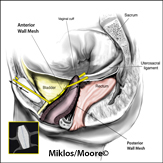
Vaginal mesh extrusion / visible mesh
Vaginal pain / Painful intercourse
Groin and/or buttocks pain
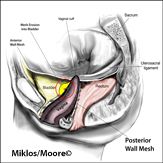
Mesh erosion in bladder or rectum
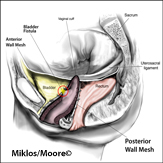
Fistula formation or abscess
Quick Contact
Call now for a Confidential Consultation! Atlanta: 678-573-6965 |
Fill out the form below to receive more information from Atlanta Center for Laparoscopic Urogynecology |