




Sacralcolpopexy Mesh Complications
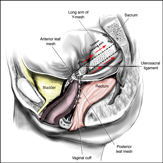
The abdominal sacral colpopexy (done through an “open” abdominal incision or laparoscopically/robotically) is the gold standard procedure to treat vaginal vault prolapse. It has the highest cure rate in the literature and has been studied for many years. It is a procedure where a Y-shaped piece of mesh is placed over the top of the vagina and down upper anterior and posterior walls of the vagina and then the other end is attached to a ligament on the sacrum. This holds up the top of the vagina, the top of the bladder and rectum. Complication rates are relatively low, however mesh complications still occur. The rates of mesh complications compared to vaginal placement of mesh seems to be lower, however it is a much more invasive operation (especially when done via laparotomy or a large open abdominal incision). Drs. Miklos and Moore recently published the largest series in the world on Laparoscopic Mesh Sacralcolpopexies and had an overall complication rate <1% (click here to see paper). However as with ANY prolapse surgery, with or without the use of mesh, complications the CAN still occur.
Types of Complications
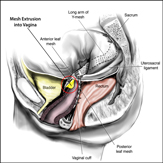
Vaginal Mesh Extrusion / Visible Mesh
Vaginal pain / Painful Sex
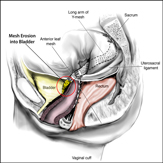
Mesh Erosion in Bladder or Rectum
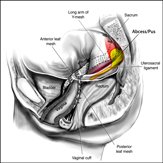
Infection / Abscess of Mesh
Quick Contact
Call now for a Confidential Consultation! Atlanta: 678-573-6965 |
Fill out the form below to receive more information from Atlanta Center for Laparoscopic Urogynecology |